This operation involves cutting out the skin cancer with a margin of healthy tissue to ensure all of the cancer is removed. It may require cutting away skin, or other soft tissue and bone.
Especially Skin Cancer on the Face, Nose and Lip
All information on the HANCA website is reviewed by our Clinical Advisory Group – a panel of Australia’s leading Head and Neck Cancer specialists. This ensures our resources are accurate, up to date, and reflect best practice in patient care and support. Meet our expert contributors and view their qualifications.
Skin cancer can be found on any part of the body. It is the most common cancer diagnosed in Australia. These cancers are either: non-melanoma skin cancers (NMSC) or melanoma. The treatment for types of skin cancer is different, so it is important to know the type of skin cancer.
Information about other types of Head and Neck Cancers can be found here.
Cancer occurs when cells become abnormal, grow uncontrollably and have the potential to spread to other parts of the body. These cells build up to form a mass (or lump).
Skin cancers occur when cells are damaged by harmful ultraviolet (UV) radiation found in light from the sun and use of solariums. Other less common causes of skin cancer can include repeated X-ray exposure, scars from burns, or occupational exposure to certain chemicals. When found early, most skin cancers can be managed with local treatment that does not have long-term side-effects.
NMSC are far more common than melanoma and are typically found on the head and neck in middle aged and older people due to long term sun exposure. People can also get skin cancers on their arms, legs and trunk.
There are two common types of NMSC:
Melanomas are less common than NMSC and can occur in younger people often as a result of previous sunburns. In Australia, melanoma is the fourth most common cancer. Sunburn causes 95% of melanomas and it is very treatable when found in its early stages
Melanoma is a cancer of melanocytes, the pigment cell in the basal layer of the skin. Like other skin cancers, melanoma is only invasive when it breaks through the bottom membrane of the skin and invades deeper tissues. Melanoma is more likely to come back (recur) and to metastasise if it has invaded the deep tissue. The chance that a melanoma will spread is related to how thick or deep it has grown into the deep tissue, presence of sores (ulceration) and other microscopic features. Melanoma can grow anywhere on the body including sun exposed skin, soles of the feet, under finger and toenails and in the eye.
Merkel cell carcinoma (MCC) (cancer of neuroendocrine cells in the skin) is a rare skin cancer that may spread to the lymph nodes. It is most commonly found in older people. Sun exposed areas, including the head and neck, arms and legs are the areas usually affected. MCC can be treated with radiation therapy alone, although surgery may also be necessary.
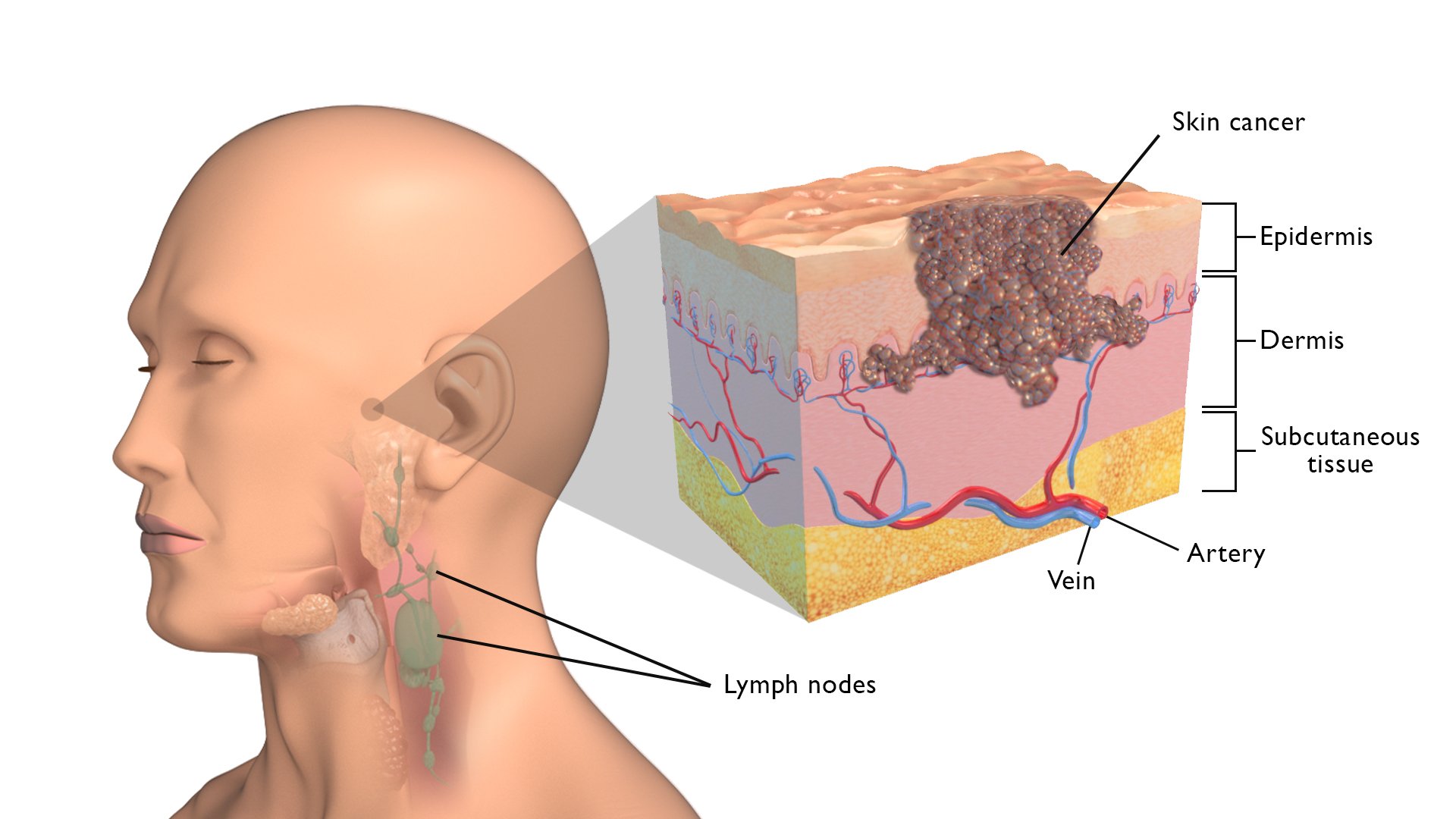
The skin is divided into two main layers. These include:
The epidermis contains three main types of cells. On the surface are flat cells, known as squamous cells. Under these are round cells called basal cells. In between the basal cells are melanocytes.
The dermis contains nerve endings, blood vessels, and oil and sweat glands. It’s held together by a protein called collagen.
The hypodermis (subcutaneous fat and connective tissue) attaches the skin to bone and muscles, as well as supplying blood vessels and nerves.
What does the skin do?
The skin is the largest organ in the body with many purposes including:
Diagram of the layers of the skin:
In Australia, sun exposure is a major risk factor for skin cancer. UV exposure in childhood and built up over a lifetime increases the risk of skin cancer, especially NMSC.
Other factors that may increase the risk of skin cancer are:
The signs and symptoms of skin cancer depend on where the cancer is, its size and how far it has spread in the body.
Symptoms and signs that indicate skin cancer may include:
You can check the parts of your skin that get exposed to sunlight (e.g. face, back and neck) for any changes. If you notice any changes or have any of the symptoms speak to your doctor.
It is important that your doctor establishes the diagnosis and type of skin cancer, assesses the extent of the cancer and whether it has spread to the lymph nodes.
To answer these questions, your doctor will need to do the following things:
Not everyone will need to have every test for skin cancer. Your doctor will recommend the tests that are right for you.
Common tests include:
If the physical examination or other procedures suggest that the cancer has spread to the lymph nodes, your doctor may order a:
The most suitable treatment for skin cancer depends on many factors. These include:
Most common skin cancers (e.g. non melanoma skin cancer) will be treated by a local excision only. Skin cancers become invasive when they break through the bottom layer of the skin (dermis) and invade into the deeper tissues. Ideally, skin cancers are treated when still within the skin - “in situ cancer”. Treatment of in situ skin cancer can be with surgery (including simple excision, curettage (also called scooping), or Moh’s surgery), radiation therapy or other treatments including liquid nitrogen therapy (freezing), cautery (using heat) or topical medications (e.g. creams or ointments).
Surgery is an important treatment for many skin cancers. For people, where the cancer has invaded the skin, there is a chance that the cancer may invade deeper structures and spread.
Your doctor will explain details of the surgery, general risks and side effects of surgery. Ask your doctor if you have questions. They may recommend:
Before starting treatment, it is important that you consider stopping smoking to reduce the risk of infection and help you fully recover after your treatment.
Surgery is an important treatment for many skin cancers. For people, where the cancer has invaded the skin, there is a chance that the cancer may invade deeper structures and spread.
The different operations that can be used for Skin Cancer are:
Local Excision (Wide Local Excision)
This operation involves cutting out the skin cancer with a margin of healthy tissue to ensure all of the cancer is removed. It may require cutting away skin, or other soft tissue and bone.
This technique is usually performed by dermatologists who have a particular interest and further specialized training. It involves serial cutting of the tumour and immediate pathologic evaluation until the margins are found to be clear of cancer. Reconstruction is often necessary.
Download PDF - Sentinel Lymph Node Biopsy
This is an investigation that may be done at the time a skin cancer is treated. It is done when there is a high risk of the cancer spreading to lymph nodes, but no nodes are obviously involved. This is most often done in people with melanoma or MCC, occasionally done for people with SCC, but rarely for BCC.
Download PDF - Reconstructive Surgery
This may be considered if a large area of tissue is removed. This operation is done by your head and neck surgeon or a surgeon who specialises in reconstructive surgery. Reconstructive surgery may involve:
Download PDF - Neck Dissection
Download PDF - Return to Activity Following Neck Dissection
This involves removal of lymph nodes from your neck. This is important in more advanced skin cancers even when there is no sign of cancer in the lymph nodes on your scan, because there is a risk of microscopic cancer in the lymph glands of the neck.
This is the removal of one of your parotid glands (pair of major salivary glands located in front of each ear) and the surrounding tissue, because of direct invasion into the gland or because of spread to lymph nodes lying within the salivary gland.
Facial Nerve Sacrifice (Radical Parotidectomy)
This is the removal of your facial nerve, which controls changes in face or expressions. It is used when a cancer in the parotid gland has spread to the nearby facial nerve.
Download PDF - Lateral Temporal Bone Surgery
This is the removal of some or all of the bone behind the ear. It is used when a cancer in the parotid gland has spread into the nearby bone.
Download PDF - Orbital Exenteration
This is the removal of the soft tissue of the eye and eyelid. It is used when a cancer has spread into the skin near the eye and cannot be treated any other way.
Treatment for skin cancer may lead to late side effects. You may not experience all of the side effects, however, talk to your doctor if you are concerned.
Treatment for skin cancer may lead to late side effects. You may not experience all the side effects, however talk to your doctor if you are concerned.
Radiation therapy can be used to treat both melanoma and NMSC. Most people with melanoma will have surgery but some people with widespread in situ melanoma, or with metastatic lymph nodes after surgery may be referred to a radiation oncologist to consider having radiation therapy.
The common type of radiation therapy for skin cancer is called external beam radiation therapy. This type of radiation therapy is applied from outside of the body. The machines used to deliver radiation therapy for skin cancer give less penetrating radiation that is because these skin cancers are on the skin surface. Some people will need deeper treatment with deeply penetrating x-rays called megavoltage photons.
Radiation therapy can be used in the following ways:
You will meet with many members of the cancer care team, who will help you learn how to look after yourself through radiation therapy, recovery and long-term follow-up. They will also talk to you about side effects and how to manage them. It may be helpful to write down questions as they come up, so you can ask anyone in your cancer care team when you see them.
You will have a planning CT scan (and sometimes other scans) with the mask on. Your radiation oncologist and radiation therapist will use these scans with all your other clinical information to develop a radiation therapy plan just for you (a personalised plan). Your plan will be checked by the radiation therapy and radiation oncology physics team, before it is ready to be used for your treatment. This whole process can take approximately 2-3 weeks.
There are many other aspects of supportive care that are available. Ask your doctor if you have any specific needs.
The side effects of radiation therapy can start during treatment and progress through treatment to peak at the end of treatment and the week after treatment. They begin to improve 2–3 weeks after the end of treatment.
Side effects associated with radiation therapy depend on:
Each person responds to radiation therapy differently. Some people may experience a few side effects while others may not experience any at all.
Common early side effects of radiation therapy may include:
Most side effects are short lived and may go away shortly after you finish radiation therapy. Some side effects may last for some time after you finish radiation therapy, and some may be permanent.
Once your radiation therapy ends, you will have regular follow-up appointments, so that your doctor can check your recovery and monitor any side effects that you may have.
Your doctor may recommend specific supportive care options to help during your treatment and recovery.
Chemotherapy for non-melanoma skin cancers is rarely used but is usually given into a vein through a needle with a cannula (tube) attached. Chemotherapy works by attacking rapidly dividing cells, such as cancer.
People with skin cancers, both melanoma and non-melanoma, may be recommended types of systemic treatment called immunotherapy. Many people with skin cancers may also be asked to take part in a clinical trial of different types of these drugs.
Being diagnosed with cancer can be overwhelming and confusing. There are a lot of information and treatment decisions to make at a distressing time for you and your family. To help you understand everything and get the information you need to make decisions about your health, consider asking the following questions to your cancer care team:
Regardless of the type of skin cancer, once a person has had one skin cancer, they are at increased risk for the same or other types of skin cancer. Regular follow-up is recommended and is best in partnership with your GP and dermatologist. It is very important that you attend follow up appointments/visits with your doctor. How often you should attend a follow up can be different, but commonly it is every 3 -4 months for the first 2 years.
If you have had a major resection, involving surgery of the lymph nodes, ongoing follow-up of this area is required, in addition to routine checking of your skin by your GP or dermatologist.
You may also need to have follow-up scans to catch any early signs of recurrence of the cancer. This may include CT, MRI and PET scanning. Remember you should contact your cancer doctor or GP if you have any concerns in the time between your visits.
Sometimes this is referred to as psychosocial aspects or survivorship. Being diagnosed with cancer and having treatment can lead to extra worries or concerns for you and the people caring for you. Depending on the treatment, you may experience any of the following:
You may get through the diagnosis and treatment for skin cancer but may find it difficult to deal with some of the side effects of treatment. Speak with your doctor about any difficulties you may be experiencing. Your doctor may give you a referral to a psychologist or another healthcare professional who can help you. Speak with your family and friends too about any concerns you may have.
You may find it helps to join a patient support group and speak with others who are having treatment for head and neck cancer. You can also find help and advice in online self-help resources such as Beyond Blue.

Reviewed by our Clinical Advisory Group
Learn more about our expert contributorsLast Updated: 01 Dec 25
On this page

Sign up to our newsletter







