
Your doctor will use a very thin flexible tube with a tiny light and camera on it to look inside your nose to see your nasopharynx.
Also known as Mouth Cancer (includes cancers of the tongue, gum and jaw)
Oral Cancer (Mouth Cancer)
Introduction
What do we mean by 'Oral Cancer'?
The colloquial term for Oral Cancer is Mouth Cancer.
Oral cancer includes cancers of the tongue, gum and jaw bone (sarcoma). If these are not the cancer type you're looking for, please explore the information about other types of Head and Neck Cancers.
Most Oral Cancers start in the cells that line the mouth (the mucosa; called squamous cell carcinomas, the same as the common types of skin cancer).
Oral Cancers can also start to grow in minor salivary glands, bone, blood vessels, nerves, and other structures. These cancers are rare and only make up less than 5% of Oral Cancers.
Cancer occurs when cells become abnormal, grow uncontrollably and have the potential to spread to other parts of the body. These cells build up to form a mass (or lump).
Watch this 3D video explainer about Oral Cancer.
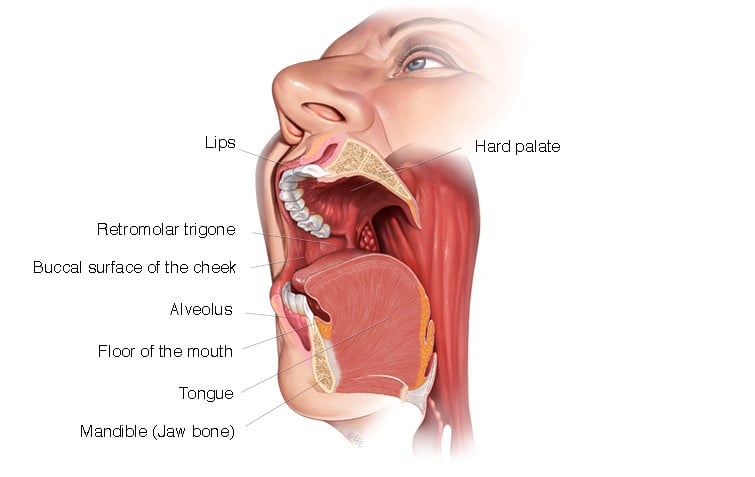
What is the Oral Cavity?
The oral (or mouth) cavity is the area between the lips and top of the throat (or oropharynx). Cancer can affect different parts of the mouth, including:
- tongue
- floor of the mouth (under the tongue and above the lower jaw)
- Maxilla and mandible (the bones that make up the upper and lower jaw)
- Gingiva (the gums)
- Buccal mucosa (inner lining of the lips and cheeks)
- Palate (the roof of the mouth, which is part of the maxilla)
- Retromolar trigone (area behind wisdom teeth)
Although the lips are part of the mouth, cancers affecting the lip are more similar to skin cancer.
What does the oral cavity do?
The oral (or mouth) cavity is important in everyday activities such as tasting, chewing and swallowing food, talking and breathing. The tongue mainly helps with eating and making foods soft enough to swallow. It also helps talking.
If any part of the oral cavity is affected by surgery (either directly through the surgery or secondarily through post-operative scarring) or radiation treatment (either as primary treatment or as a post operative adjuvant therapy), any of these functions may be adversely affected.
If the tongue cannot move properly, either because of loss of muscle from surgery, or getting stuck from scarring and limiting movement, then talking and the ability to eat can be affected greatly.
The jaw bones help keep the shape of the face and gives a strong bony frame to allow room for chewing.
Oral Cavity
What causes Oral Cancer?
Doctors often can’t explain why a person gets cancer. But we do know what makes some cancers more likely.
The two main causes of Oral Cancer are:
-
smoking (cigarettes, cigars or pipes) or using ‘smokeless’ tobacco (snuff and chewing tobacco) If a person smokes or has smoked in the past, they have a higher risk of getting Mouth Cancer than someone who has never smoked.
-
drinking alcohol — If a person drinks a lot of alcohol over many years, they have a higher risk of getting Mouth Cancer, especially combined with smoking.
Three out of four people with Oral Cancer have been a smoker or consumed alcohol regularly for a number of years.
Get information about quitting smoking and reducing how much alcohol you drink.
Other factors that may increase the risk of Oral Cancer are:
- being male – in Australia men are more likely than women to get Oral Cancer
- age – most Oral Cancers (about 90%) are in people aged over 50 years
- previous diagnosis of Oral Cancer
- using mouthwash containing alcohol, over a number of years
- using betel nut (betel quid) – Oral Cancers are more common in parts of Asia where betel quid is chewed
- lichen planus – an inflammatory condition that causes white and red patches in the mouth (although less than 1 in 100 people with this condition develop Oral Cancer)
- a poor diet low in fruit and vegetables
- broken and sharp teeth rubbing on the tongue and cheek
Signs and Symptoms of Mouth Cancer
The signs and symptoms of Oral Cancer depend on where the cancer is in the mouth, its size and how far it has spread in the body.
Common signs and symptoms include:
- a sore (like an ulcer) or lump in the mouth that doesn’t improve, or increases in size
- pain in the mouth or ear
- white or red patches on the gums, tongue or mouth
- unusual bleeding or numbness in the mouth
- trouble chewing or swallowing food, or moving the tongue
- difficulty opening the mouth
- a lump in the neck
- loose teeth or dentures that no longer fit.
Most often these symptoms are not from Oral Cancer. However, if you have any of these symptoms for more than a few weeks, talk to your doctor as early as possible. They may be able to help diagnose and treat you.
Tests for Mouth Cancer
It is important that your doctor establishes the diagnosis of Oral Cancer, assesses the size of the cancer and whether it has spread to the lymph nodes in the neck or elsewhere in the body.
To answer these questions your doctor may need to do the following things:
- talk with you about your medical history. This includes signs you may have noticed, any other health conditions, medications that you are taking, and whether you smoke or drink alcohol
- perform a physical examination by feeling and looking inside your mouth, throat and neck
- order diagnostic tests, which may include Xrays, CT scans, MRI scans, PET scans and biopsy.
Not everyone will need to have every test for Oral Cancer. Your doctor will recommend the tests that are right for you. The most common tests include:
This involves taking a small piece (sample) from the cancer. The sample is then examined under a microscope to check for cancer cells. This is often the only sure way to tell if you have cancer. Your doctor may recommend one of the three types of biopsies:
-
Excision biopsy: This is when the doctor removes the cancer completely. This will usually be done for small cancers in the clinic or the operating room.
-
Incision biopsy: This is when the doctor removes a small piece of tissue using a surgical knife. This can be done in the clinic using local or general anaesthesia, so that you don't feel any pain. Depending on the size and location of the biopsy, you may need stitches. There may be some bleeding after the biopsy. If you take blood thinners, you may need to stop these for a few days before the biopsy.
-
Needle biopsy (Fine Needle Aspiration or FNA): This is used when there is a lump (enlarged lymph node) in the neck that could have cancer cells in it. During the procedure, your doctor will take some cells from the lump using a needle. Usually this is done with guidance from an ultrasound to make sure the needle is in the right spot. You may feel a bit uncomfortable during the biopsy.
This uses X-rays to take pictures of the inside of the body. If the person has cancer, a CT scan can help the doctor to see where it is, measure how big it is, and if it has spread into nearby organs or other parts of your body.
PET (Positron Emission Tomography) SCAN
This is a whole body scan that uses a radioactive form of sugar, which can show if oral cancer has spread to the lymph nodes or elsewhere in the body. Many patients with oral cancer do not need a PET scan.
MRI (Magnetic Resonance Imaging) Scan
This uses magnetic fields to take pictures of the inside of the body. This helps the doctor see how far a cancer has grown into the tissue around it. Not all people with oral cancer need a MRI scan.
This X-ray will help the dental team assess your oral health.
Although there is no blood test specific for Oral Cancer, other blood tests are important to check your health and fitness for treatment.
Pathology tests involve the laboratory testing of blood, body fluids and tissues. There are three common pathology tests for head and neck cancer.
Cytology
Cytology uses a needle to remove cells so they can be looked at under a microscope. It is often used if you have swollen (enlarged) lymph glands, neck cysts and thyroid nodules.
Histopathology
Histopathology is when part or all of the cancer cells are looked at under a microscope. The cancer cells are usually collected during a biopsy and sent to a doctor trained in looking at cells in the body (pathologist) for testing. The pathologist will be able to tell your doctor the type of cancer, its grade, and other details that will help your doctor work out the best treatment for your type of cancer.
Blood Tests
Blood tests are not typically used to diagnose of screen for most types of head and neck cancer. There are some blood tests that can be used to look for certain types of thyroid cancer. Sometimes your healthcare team will ask you to have blood tests to make sure that your blood, kidneys, and liver are working normally.
Treatment Options for Mouth Cancer
Following a diagnosis of Oral Cancer, your cancer care team will discuss the treatment options that are suitable for you. This is also a good time to consider if you would like a second opinion.
The most suitable treatment of oral cancer depends on many things including:
- size and location of the cancer
- whether it has spread
- personal factors (e.g. age, general health and treatment history)
- types of treatment available (and whether there are any clinical trials that are suitable for you)
- your preferences for treatment.
While some people can be treated with surgery alone, others may need extra treatment after surgery to reduce the risk of the cancer returning. Your cancer care team will decide whether it is necessary for you based on a detailed report on the cancer from the pathologist 1–2 weeks after surgery.
Adding another type of treatment after surgery is called adjuvant therapy. This can be either radiation therapy alone or combined with chemotherapy (called chemoradiation), which is typically started about 4-6 weeks after surgery to allow recovery and for planning purposes.
The treatment itself usually lasts about 6 weeks.
Surgery for Oral Cancer
There are a number of different operations that can be used to remove Oral Cancer. The type of operation used will depend on the size of the cancer and where it is.
How can I Prepare for the Surgery?
Your doctor will explain details of the surgery, general risks and side effects of surgery. Ask your doctor if you have questions. They may recommend:
- stopping blood thinners (e.g. aspirin) before surgery to reduce the risk of bleeding
- special stockings to reduce the risk of blood clots
- early mobilisation (i.e. not staying in bed) to reduce the risk of blood clots and chest infection
- antibiotics to lower the risk of wound infection.
If you smoke, it is important that you consider stopping smoking before starting treatment to help reduce the risk of infection and help you recover after your treatment.
Surgical Procedures
The different options for oral cancer include:
This involves removing part of, or all of the tongue. It is used if the cancer is growing in the tissue of the tongue.
This involves removing part of the lower jaw (mandible). It is used if the cancer has spread into the bone of the jaw or is next to the jaw.
This involves removing part of the upper jaw (maxilla), in the roof of the mouth. It is used when the cancer is affecting the roof of the mouth or upper gums.
This involves cutting the jaw bone to allow better access to the cancer in the mouth. This may be needed if the cancer is further back and difficult to reach through the mouth. The jaw is put back together at the end of the operation with titanium plates.
This involves removing lymph nodes from the neck. It is used when oral cancer has spread to the lymph nodes in the neck or there is a risk of cancer in the lymph nodes of the neck.
Reconstructive Surgery (Soft Tissue Free Flap or Bony Free Flap)
Download PDF - Reconstructive Surgery (Soft Tissue Free Flap)
Download PDF - Reconstructive Surgery (Bony Free Flap)
This may be considered if a large area of tissue is removed. This may involve taking tissue from another part of the body called a free flap repair. If your jaw has been removed, bone from another part of the body may be used to replace your jaw bone. This operation is carried out by a surgeon who specialises in reconstructive surgery, your head and neck surgeon or another surgeon.
A tracheostomy is used to create an opening in the trachea (windpipe) in the lower neck, where a tube is inserted to allow air to flow in and out, when you breathe. This is used as swelling after major head and neck surgery may affect your ability to breathe. The tracheostomy tube is usually removed within a week of surgery once normal breathing is possible.
- A gastrostomy tube (called a PEG tube) goes through the skin and the muscles of your abdominal wall into the stomach. Gastrostomy is recommended if feeding is needed for a medium to longer time (months or years).
- A nasogastric tube goes through the nose down into the stomach. Nasogastric feeding is used for short time (days or weeks).
Radiation Therapy for Oral Cancer
The most common radiation therapy approach for Oral Cancer is called external beam radiation. This type of radiation therapy applies radiation from outside the body.
Radiation therapy can be used in the following ways:
Definitive
This is when radiation therapy is used without surgery to cure oral cancer, often in combination with chemotherapy. This approach has a very limited role in oral cancer, as most patients are best treated with surgery as first-line therapy. It may however be used if a patient is not a candidate for surgery.
Adjuvant
This is when radiation therapy is given after surgery, to kill cancer cells that may not have been taken out during surgery. Adjuvant radiation therapy can also be given in combination with chemotherapy (this is called concurrent chemoradiation). The decision to give radiation therapy, either alone or in combination with chemotherapy, is based on the pathology results after surgery. The aim is to lower the risk of the cancer returning in the mouth or neck, but not all patients may need this.
Palliative
In cases where a cure is not possible, radiation therapy is used to relieve symptoms of advanced oral cancer. Symptoms that may require palliative radiation therapy include pain, bleeding, breathing and trouble swallowing.
Side effects of Radiation Therapy
The side-effects of radiation therapy start around two weeks into treatment and progress through treatment to peak in the last week or just after treatment ends. The side effects start to improve 2-3 weeks after the end of treatment.
Side effects associated with radiation therapy depend on:
- the dose of radiation therapy
- the area being treated
- whether or not chemotherapy is added to the radiation.
Each person responds to radiation therapy differently. Some people may experience a few side effects while others may not experience any at all. The following are some common side effects of radiation therapy.
- tiredness
- skin irritation in the treated area e.g. redness, dryness and itching, weeping skin, scaling or sometimes skin breakdown (sores)
- dry mouth and throat due to lack of saliva (called xerostomia)
- changed taste (usually a loss of taste or sometimes an unpleasant taste in the mouth)
- pain on swallowing or difficulty with swallowing
- loss of weight.
Most side effects are short lived and may go away within 4–6 weeks of finishing radiation therapy. Some side effects may last for months after you finish radiation therapy and some may be permanent.
Once your radiation therapy ends, you will have regular follow-up appointments so your cancer care team can check your recovery, make sure the cancer has not returned, and monitor and treat any side effects that you may have.
Your doctor may recommend that you receive some specific supportive care to help during your recovery such as help with changes in speech, voice or swallowing, diet and nutrition and teeth and mouth care.
Chemotherapy for Oral Cancer
Chemotherapy works by destroying or damaging cancer cells. For Mouth Cancer, it is usually given into a vein through a needle with a cannula (tube) attached.
There are a number of ways that chemotherapy may be used to treat Mouth Cancers including:
Adjuvant
This is when chemotherapy is given after surgery in combination with radiation therapy (called concurrent chemoradiation). It may be given once every 3 weeks or once a week throughout the duration of radiation therapy. This makes the radiation more effective at killing cancer cells but also leads to more side effects in most people. Unlike chemotherapy for many other cancers, most people do not lose their hair or have severe nausea and vomiting.
Neo-adjuvant
This is when chemotherapy is given before surgery or radiation therapy to help shrink large cancers, making them easier to remove during surgery, or target with radiation therapy. This is very rarely used for oral cancer but may be used for sarcomas.
Palliative
This is used when the cancer is incurable. The cancer may be too large or has spread too much to be removed by surgery. Palliative chemotherapy helps to slow the growth of cancer and reduce symptoms. It is important to remember that palliative chemotherapy is not as intense as other types and is much less likely to have significant side effects.
Before you start treatment, your medical oncologist will choose one or more chemotherapy medications that will be best to treat the type of cancer you have.
The chemotherapy medications your doctor chooses may depend on:
• whether the treatment is curative or palliative
• when it is used
• your medical history.
Side Effects of Chemotherapy
The side effects of chemotherapy depend on the medication used and and how much you is given by your doctor (the dose). The most common medications used are called cisplatin, carboplatin and cetuximab.
Each person responds to chemotherapy differently. Some people may experience a few side effects while others may not experience any at all. The following are common side effects of chemotherapy:
- a feeling of wanting to vomit (nausea) or vomiting
- more side effects of radiation, if you have chemotherapy at the same time as radiation
- loss of feeling in the fingers and toes
- kidney damage (caused by some medications)
- hearing loss/reduction
- ringing in the ears
- rash
- higher risk of infection (if the chemotherapy reduces the number of white cells in the blood)
Most of these side effects are short lived and may go away once you finish chemotherapy. Some side effects can take months or years to improve or may be permanent.
Immunotherapy
Immunotherapy, in combination with chemotherapy may be considered if the cancer has spread, returned after treatment, or is not responding to standard therapies like chemotherapy or radiation.
Your treating medical oncologist will discuss the best treatment approach with you.
Once your treatments end, you will have regular follow-up appointments so that your doctor can check your recovery, make sure the cancer has not returned and monitor and treat any side effects that you may have.
Your doctor may recommend that you receive some specific supportive care to help during your recovery. Further information about supportive care is available on the website.
Once your treatments end, you will have regular follow-up appointments so that your doctor can check your recovery, make sure the cancer has not returned and monitor and treat any side effects that you may have.
Your doctor may recommend that you receive some specific supportive care to help during your recovery.
Questions to Ask
- Exactly what type of Oral Cancer do I have? Where is it located?
- Why did I get this cancer? Is it related to smoking or alcohol?
- Why did I get this cancer? Is it related to the HPV virus?
- What stage is the cancer?
- What are my treatment options? Which treatment do you recommend for me and why?
- Have you discussed my case at a Multidisciplinary Team meeting and what were the recommendations?
- Who will be part of the cancer care team, and what does each person do? Should I see another specialist before treatment, such as a radiation oncologist, medical oncologist, plastic surgeon, dentist, dietitian or speech pathologist?
- What are the possible side effects of treatment in the short- and long-term? How can they be prevented or managed?
- Will the treatment affect my ability to eat, swallow, or speak? Will I need a feeding tube?
- What will happen if I don't have any treatment?
- How much will the treatment and/or operation cost? Will Medicare or my health insurance cover it?
- What follow-up tests will I need? How often will they be?
- Am I suitable for any clinical trials?
- What lifestyle changes (diet, exercise) do you recommend I make?
- Who can I call if I have any problems or questions?
- Where can I find emotional support for me and my family? Is there a support group or psychologist you can recommend?
- If I wanted to get a second opinion, can you provide all my medical details? Do you mind if I get a second opinion?
Follow-up Care
You will need regular check-up of your mouth, throat and neck after treatment for oral cancer. This will include a physical exam. Some people may also need imaging such as CT, MRI and PET scans, during follow-up. It is important to keep up with follow-up appointments to make sure that if the cancer comes back, it is caught early and can be treated. If you have any concerns between appointments you should contact your doctor.
People who smoke and/or drink alcohol can reduce the risk of their cancer coming back or getting a new cancer if they quit smoking and reduce the amount of alcohol they drink. Ask your cancer care team for advice if this applies to you.
Importance of ongoing Dental Care
A dentist plays an important role in your head and neck cancer treatment. Side-effects can often be prevented or reduced through regular dental check-ups before, during and after cancer treatment.
After your treatment, you should visit the dentist every six months for a check-up because the side effects of radiation therapy on your teeth can last for your whole life.
Mental health for people with Cancer
Sometimes this is referred to as psychosocial aspects or survivorship.
Being diagnosed with cancer and having treatment can lead to extra worries or concerns for you and the people caring for you. Depending on the treatment, you may experience any of the following:
- low mood or depression
- anxiety
- disfigurement
- difficulties with eating
- difficulties with speaking
- changes in sexual activity
You may have got through the diagnosis and treatment for mouth cancer, but you may be finding it difficult to deal with some of the side effects of treatment. Speak with you doctor about any difficulties you may be experiencing. Your doctor may give you a referral to a psychologist or another healthcare professional who can help you.
For more information about coping with cancer visit Cancer Council Australia.









Reviewed by Clinical Advisory Group
Learn more about our expert contributorsLast Updated: 30 Sep 25
On this page
