
Your doctor will use a very thin flexible tube with a tiny light and camera on it (endoscope) to look at your throat and voicebox.
All information on the HANCA website is reviewed by our Clinical Advisory Group – a panel of Australia’s leading Head and Neck Cancer specialists. This ensures our resources are accurate, up to date, and reflect best practice in patient care and support. Meet our expert contributors and view their qualifications.
Most Salivary Gland Cancers are found in the parotid glands. The parotid glands contain glands of the immune system (lymph nodes). If this is not the cancer type you're looking for, please explore the information about other types of Head and Neck Cancers.
Cancer occurs when cells become abnormal, grow uncontrollably and have the potential to spread to other parts of the body. These cells build up to form a mass (or lump).
Most salivary gland tumours are not life threatening (malignant) and are called benign tumours. Some benign tumours can become malignant over time.
Cancer of the parotid glands may either start:
A small number of Salivary Gland Cancers start in the submandibular, sublingual and minor salivary glands lining the mouth and throat.
There are many different types of primary Salivary Gland Cancer. Each of these cancer types behave differently. Some high-grade salivary tumours spread along nerves or to lymph nodes and to other parts of the body. Low-grade tumours are less likely to spread.
Watch a 3D video explainer about Salivary Gland Cancer:
The salivary glands make spit (saliva) and releases it into the mouth to keep the mouth and throat moist, and help with swallowing and digesting food.
There are major (large) and minor (small) salivary glands. There are three pairs of major salivary glands: the parotid gland, submandibular glands and sublingual glands.
Parotid Gland
The parotid glands are found just in front of the ears and behind the jaw. They move saliva into the mouth through a tube called the parotid duct. This tube opens on the inside of the cheek, near the upper molar teeth. The nerve that controls the facial muscles (called the facial nerve), runs through the parotid gland. This nerve makes you smile, frown, close your eyes and raise your eyebrows.
The parotid gland is the largest salivary gland and where most Salivary Gland Cancers occur.
The parotid glands also contain lymph nodes (bean shaped glands that are part of the immune system’s defence against infections). Sometimes skin cancers, can spread to the lymph nodes inside the parotid glands. Most parotid gland tumours are not cancers and are called benign tumours.
Submandibular and Sublingual Glands
The submandibular glands lie under the jawbone, one on each side. They release saliva into the mouth through a duct (tube) that opens in the floor of the mouth, under the tip of the tongue. Three important nerves are found next to these glands –the hypoglossal nerve, lingual nerve and marginal branch of the facial nerve. These nerves give movement, feeling and taste to the tongue and move the lower lip. Tumours of the submandibular gland can be benign (not cancer) or malignant (cancer).
The sublingual glands lie under the tongue, one on each side. They release saliva into the submandibular duct and are near the lingual nerves which give feeling and taste to the front of the tongue. The sublingual glands are the smallest of the major salivary glands and rarely develop tumours, but tend to be malignant (cancer) when they do develop.
Minor Salivary Glands
There are hundreds of minor salivary glands throughout the mouth and throat. They can be found inside the mouth, just under the surface including the lips, cheeks and top of the mouth (soft palate). The minor salivary glands can also develop tumours, which can be benign or malignant.
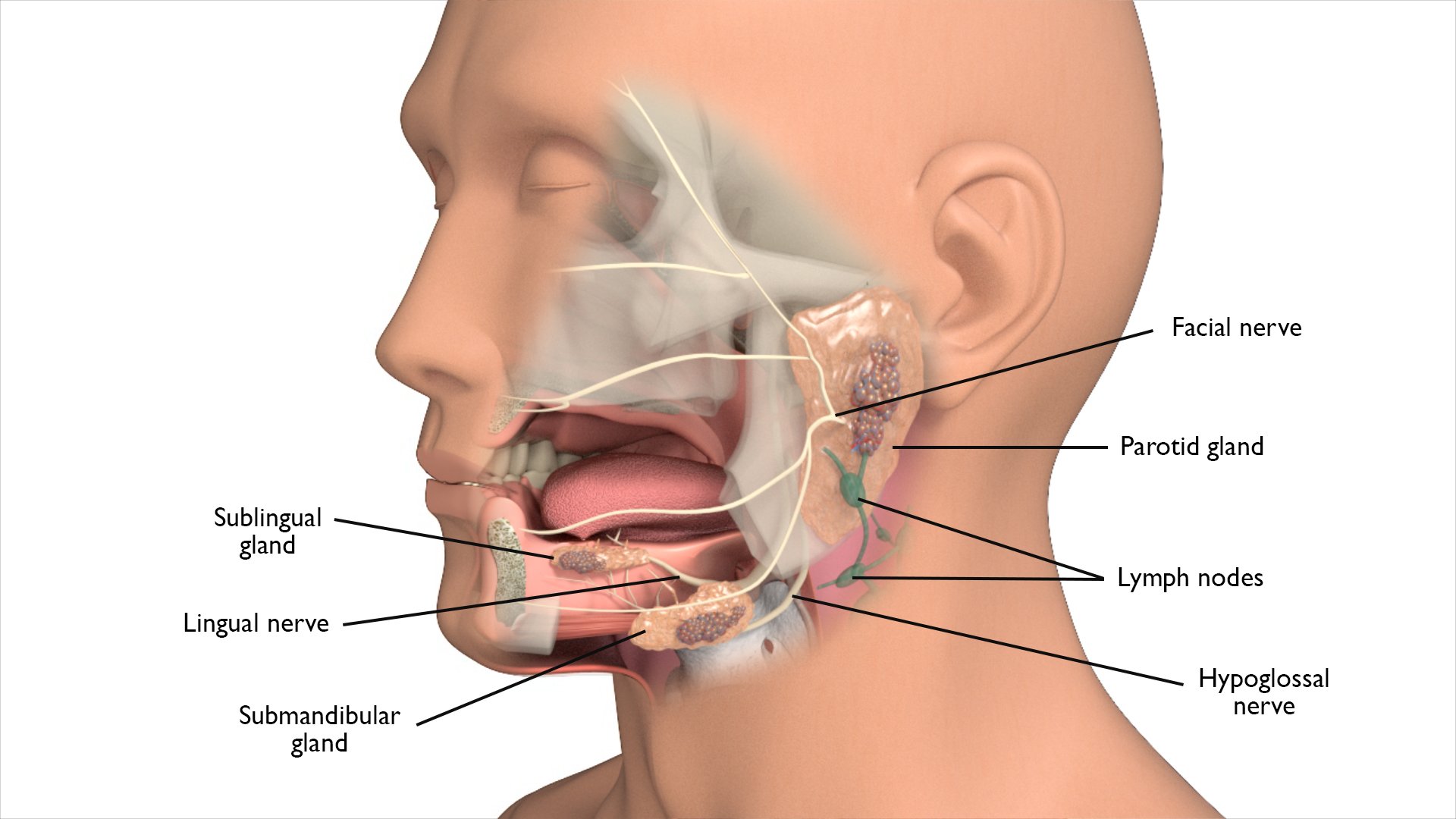
Diagram of the salivary glands and surrounding areas:
Doctors often can’t explain why a person gets cancer. However, factors that may increase the risk of Salivary Gland Cancer include:
Other factors, such as using mobile phones and exposure to industrial chemicals, have not been proven to increase the risk of Salivary Gland Cancer.
The signs and symptoms of Salivary Gland Cancer depend on where the cancer is, its size, and how far it has spread in the body.
Common signs and symptoms include:
Most of these are also signs and symptoms of other conditions. However, if you have any of these symptoms for more than a few weeks, speak with your doctor as early as possible. They may be able to help diagnose and treat you.
It is important that your doctor establishes the diagnosis of Salivary Gland Cancer, assesses the size of the cancer and whether it has spread to the lymph nodes in the neck or elsewhere in the body.
To answer these questions, your doctor will need to do the following things:
Not everyone will need to have every test for Salivary Gland Cancer . Your doctor will recommend tests that are right for you.
Common diagnostic tests include:
Your doctor will use a very thin flexible tube with a tiny light and camera on it (endoscope) to look at your throat and voicebox.
This involves taking a small piece (sample) from the cancer. The sample is then examined under a microscope to check for cancer cells. This is often the only sure way to tell if you have cancer. Diagnosis of salivary gland cancers can be very difficult and, sometimes, a definite diagnosis cannot be made until the whole cancer is removed.
Your doctor may recommend an incision biopsy or a needle biopsy.
This uses X-rays to take pictures of the inside of the body. If the person has cancer, a CT scan can help the doctor see where it is, measure how big it is, and if it has spread into nearby organs or other parts of your body.
MRI (Magnetic Resonance Imaging) Scan
This uses magnetic fields to take pictures of the inside of the body. MRI is very good at looking at the salivary glands and determining whether any cancer is spreading along the nerves.
PET (Positron Emission Tomography) Scan
This is a whole body scan that uses a radioactive form of sugar which can show if salivary gland cancer has spread to other parts of the body. Low-grade salivary gland cancer may not show up on PET scan, because it tends to grow slowly.
This uses sound waves and helps the doctor to see salivary gland cancer. An ultrasound scan can show if a cancer is benign or malignant. Ultrasound scans are also often used to guide a needle biopsy and to look at lymph nodes.
Following a diagnosis of Salivary Gland Cancer, your cancer care team will discuss treatment options that are suitable for you. This is also a good time to consider if you would like a second opinion.
The most suitable treatment of Salivary Gland Cancer depends on many things. These include:
Surgery is often the main treatment for Salivary Gland Cancer. This involves cutting the cancer out and, for some patients, taking out the lymph nodes.
A week or two after surgery, your pathologist will give a detailed report on the cancer. This will be used by your cancer care team to decide if you need more treatment to reduce the risk of the cancer coming back. This treatment may be radiation therapy alone or radiation combined with chemotherapy (chemoradiation) and, occasionally, it may be radiation therapy followed by chemotherapy.
Adding another treatment after surgery is called adjuvant therapy. Adjuvant therapy usually starts about 4–6 weeks after surgery so that you have time to recover from your surgery. Adjuvant therapy usually lasts for about 6 weeks.
Salivary Gland Cancer can cause physical changes while its treatment can cause side effects. Some of these physical changes and side effects will go away soon after treatment, while others may be long-term or permanent.
Your doctor will explain details of the surgery, general risks and side effects of surgery. Ask your doctor if you have questions. They may recommend:
Before starting treatment, it is important that you consider stopping smoking to reduce the risk of infection and help you fully recovery after your treatment.
There are a number of different types of operations that can be used to remove Salivary Gland Cancer. The type of surgery used will depend on the size and the location of the cancer.
The different operations that can be used for Salivary Gland Cancers are:
This is removal of one or both of the parotid glands (pair of major salivary glands located in front of each ear) and the surrounding tissue.
Download PDF - Submandibular Gland Surgery
This is removal of the submandibular glands (located beneath the floor of your mouth) and some of the surrounding tissue and/or bone.
Download PDF - Sublingual Gland Surgery
This is removal of the sublingual glands (located in the mouth) and some of the surrounding tissue.
Facial Nerve Sacrifice (Radical Parotidectomy)
Download PDF - Facial Nerve Sacrifice (Radical Parotidectomy)
This is removal of facial nerve, which controls facial expression. It is performed when a cancer in the parotid glands has spread to surrounding facial nerve.
Download PDF - Lateral Temporal Bone Surgery
This is the removal of some or all of the bone in the temple and behind the ear. It is used when a cancer in the parotid glands spreads into the nearby bone.
Download PDF - Neck Dissection
Download PDF - Return to Activity Following Neck Dissection
This involves taking out the lymph nodes from the neck. It is used when cancer of the salivary glands has spread to the lymph nodes in the neck or there is a risk of cancer in the lymph nodes of the neck.
Reconstructive Surgery - Soft Tissue Free Flap
Download PDF - Reconstructive Surgery - Soft Tissue Free Flap
This may be considered if you have a large area of tissue removed. This may involve taking tissue from another part of the body, this is called a free flap repair. This operation is carried out by a surgeon who specialises in reconstructive surgery, your head and neck surgeon or another surgeon.
A tracheostomy is used to create an opening in the trachea (windpipe) after major head and neck surgery. A tube is inserted into the opening to help you breathe until normal breathing is possible.
Download PDF - Dental Extraction
Tooth extractions may be recommended to remove any broken or infected teeth before radiation therapy. This is important because removal of unhealthy teeth after radiation therapy can cause problems with the jaw bone.
Treatment for Salivary Gland Cancer may lead to a number of side effects. Possible side effects depend on the surgical approach that best suits your individual cancer. It depends on whether you need to have lymph nodes removed from the neck. You may not experience all of the side effects. Speak with your doctor if you have any questions or concerns about treatment side effects.
The most common approach of radiation therapy for Salivary Gland Cancer is called external beam radiation. This type of radiation therapy applies radiation from outside the body.
Radiation therapy can be used in the following ways:
Definitive
This is when radiation therapy is used on its own without surgery to cure Salivary Gland Cancer. It is used in Salivary Gland Cancer when surgery is not a treatment option.
Adjuvant
This is when radiation therapy is given after surgery, to kill cancer cells that may not have been taken out during surgery. It can be used either on its own or at the same time as chemotherapy (chemoradiation), to make it more effective. The decision to give radiation therapy, either alone or with chemotherapy, is based on the pathology results after surgery. The aim of adjuvant radiation therapy is to reduce the risk of Salivary Gland Cancer coming back. Not everyone will require adjuvant radiation therapy.
Palliative
In cases where a cure is not possible, radiation therapy is used to relieve symptoms of advanced Salivary Gland Cancer. Symptoms that may require palliative radiation therapy include pain, bleeding, breathing and trouble swallowing.
You will meet with many members of the cancer care team, who will help you learn how to look after yourself through radiation therapy, recovery and long term follow-up. They will also talk to you about side effects and how to manage them. It may be helpful to write down questions as they come up, so you can ask anyone in your cancer care team when you see them.
Radiation Therapy Mask-Making and Simulation
Teeth and Mouth Care
You might need to have some of your teeth taken out, this will depend on the area being treated and the dose of radiation therapy. It is important to take out any broken or infected teeth before radiation therapy. Taking out unhealthy teeth after radiation therapy can cause problems with the jaw bone. Further information about removing teeth and teeth and mouth care can be found here.
Diet, Nutrition and the Role of your Dietitian
Your cancer and its treatment can make it hard to eat and drink. Your doctor will recommend you see a dietitian to maximise your nutrition during treatment as well as while you are recovering. Sometime feeding tubes may be recommended depending on the area being treated and the dose of radiation therapy.
There are two common types of feeding tubes:
Speech, Voice and Swallowing
Your cancer and its treatment can make swallowing and speech difficult. Your doctor will recommend you see a speech pathologist, who can help you with ways to manage swallowing and communication difficulties, during and after treatment.
There are many other aspects of supportive care that are available, ask your doctor if you have any specific needs.
The side-effects of radiation therapy start around two weeks into treatment and progress through treatment to peak in the last week or just after treatment ends. The side effects start to improve 2-3 weeks after the end of treatment.
Side effects associated with radiation therapy depend on:
Each individual responds to radiation therapy differently. Some people may experience a few side effects while others may not experience any at all. The following are some common side effects of radiation therapy.
Common side effects of radiation therapy include:
Most side effects are short lived and may go away within 4–6 weeks of finishing radiation therapy. Some side effects may last for months after you finish radiation therapy and some may be permanent.
Once your radiation therapy ends, you will have regular follow-up appointments so your cancer care team can check your recovery and monitor any side effects that you may have. Your doctor may recommend some specific supportive care options to help during your recovery, such as help with changes in diet, teeth and mouth care and speech or swallowing.
Chemotherapy works by destroying or damaging cancer cells. For Salivary Gland Cancer, it is usually given into a vein through a needle with a cannula (tube) attached.
There are a number of ways that chemotherapy may be used to treat Salivary Gland Cancer including:
Adjuvant
This is when chemotherapy is given after surgery and is usually combined with radiation therapy (chemoradiation). It is usually given once a week during radiation therapy. Adding chemotherapy makes the radiation more effective at destroying cancer cells, but also leads to increased side effects for most patients
Neo-adjuvant
This is when radiation therapy is given before surgery or radiation therapy. It is used to shrink large cancers so they are easier to remove during surgery or target with radiation therapy. Neoadjuvant chemotherapy is rarely used for Salivary Gland Cancer.
Palliative
This is given when the cancer is incurable, because the cancer is too big or has spread too far to be removed by surgery. Even if a cancer is incurable, some patients feel better from palliative chemotherapy as it slows the growth of the cancer, and can relieve or prevent symptoms.
Before you start treatment, your medical oncologist will choose one or more chemotherapy medications that will be best to treat the type of cancer you have.
The chemotherapy medications your doctor chooses may depend on:
The side effects of chemotherapy depend on the medication used and its dose. The most common medications used are called cisplatin, carboplatin and fluorouracil (5-FU).
Each individual responds to chemotherapy differently. Some people may experience a few side effects while others may not experience any at all.
The following are common side effects of chemotherapy:
Most of these side effects are short lived and go away once you finish chemotherapy. Some side effects like hearing loss, may be permanent.
Once your treatments end, you will have regular follow-up appointments so that your doctor can check your recovery, make sure the cancer has not returned and monitor and treat any side effects that you may have. Your doctor may recommend that you receive some specific supportive care to help during your recovery.
You will need regular checkups of your face, mouth, throat and neck after treatment for Salivary gland Cancer. This will include a physical exam. Some patients may also need imaging of their mouth using CT, MRI and PET scans, however, most patients with salivary gland cancer won't need this. It is important to see your cancer care team for regular follow-up visits to make sure that if the cancer comes back it is caught early and can be treated. If you have any concerns between appointments you should contact your doctor. Ask your doctor whether this is needed for you.
Sometimes this is referred to as psychosocial aspects or survivorship.
Being diagnosed with cancer and having treatment can lead to extra worries or concerns for you and the people caring for you. Depending on the treatment, you may experience any of the following:
You may have got through the diagnosis and treatment for salivary gland cancer, but you may be finding it difficult to deal with some of the side effects of treatment. Speak with you doctor about any difficulties you may be experiencing. Your doctor may give you a referral to a psychologist or another healthcare professional who can help you. Speak with your family and friends too about any concerns you may have.
You may find it helps to join a patient support group and speak with others who are having treatment for head and neck cancer.
You can also find help and advice in online self-help resources such as beyondblue
Further information about coping with cancer is available here

Reviewed by our Clinical Advisory Group
Learn more about our expert contributorsLast Updated: 30 Sep 20
On this page

Sign up to our newsletter







