
Your doctor will use a very thin flexible tube with a tiny light and camera on it to look inside your nose.
Nose Cancer (Nasal, Sinus Cancer)
Also known as Nasal Cancer, includes Sinus Cancer
Introduction
What is Nose or Nasal Cancer?
Nasal Cancer is a type of Head and Neck Cancer in the nose and nasal cavity. It also covers Sinus Cancer.
If it's not the cancer type you're looking for, please explore the information about other types of Head and Neck Cancers.
Different types of cancer can develop from the different kinds of cells in the nasal cavity and paranasal sinuses. The most common are called squamous cell carcinoma (arising from the lining of the nasal cavity and the paranasal sinuses) and adenocarcinoma (arising from the small gland cells throughout the sinuses).
Cancer occurs when cells become abnormal, grow uncontrollably and have the potential to spread to other parts of the body. These cells build up to form a mass (or lump).
Nasal and paranasal cancers are relatively rare. The most common location of paranasal sinus cancer is the maxillary sinus.
Watch this 3D video explainer about Nasal and Sinus Cancer:
What is the Nasal Cavity and Paranasal Sinuses?
The nasal cavity is the large, air-filled space behind the nose. Paranasal sinuses are small air-filled spaces at the front of the skull, and surrounding the nasal cavity. They are found on the cheeks (the maxillary sinuses), above the eyes (the frontal sinuses), between the eyes (the ethmoidal air cells or sinuses) and behind the ethmoidal aircells (sphenoid sinuses).
What do the Nasal Cavity and Paranasal Sinuses do?
The nasal cavity warms and moistens the air we breathe and helps filter out dust and other harmful bits in the air. It runs back from the nostrils, above the roof of the mouth and curves down to connect with the mouth at the back of the throat.
The paranasal sinus air cavities give your voice its clarity and tone and lighten the weight of the skull.
The nasal cavity is the main sensory organ responsible for the human sense of smell. It consists of specific receptors (olfactory) which are responsible for transmitting odours into neural impulses.
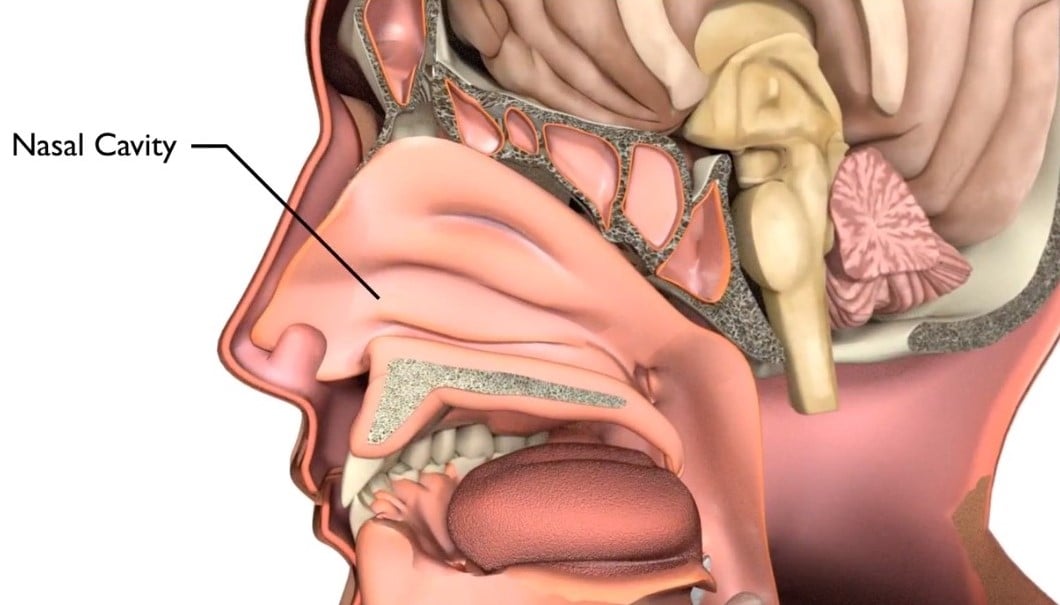
Diagram of the nose and surrounding areas
What causes Nose Cancer?
Doctors can’t always explain why a person gets cancer. But we do know what makes some cancers more likely.
The main causes of nose and paranasal sinus cancers are:
- Smoking (cigarettes, cigars or pipes) or using ‘smokeless’ tobacco (snuff and chewing tobacco) If a person smokes or has smoked in the past, they have a higher risk of getting nasal and paranasal sinus cancer than someone who has never smoked. Get information about quitting smoking.
- Drinking alcohol — If a person drinks a lot of alcohol over many years, they have a higher risk of getting nasal and paranasal sinus cancer, especially combined with smoking. Get information about reducing how much alcohol you drink.
- Breathing in certain chemicals or dust that may cause cancer including wood dust (hard and soft wood), leather dust (e.g. shoe making), chromium, nickel, heavy metal exposure, formaldehyde, cloth fibres (e.g. textile manufacturing) and mineral oils (used in metal work and printing.
Other factors that may increase the risk of nose and paranasal sinus cancer are:
- Being male – in Australia nasal and paranasal sinus cancers are twice as common in men compared to women
- Age — most nasal and para nasal sinus cancers are common in people aged 45 years and over
Symptoms and Signs of Nose Cancer
The signs and symptoms of Nose Cancers depend on where the cancer is, its size and how far it has spread in the body.
Common signs and symptoms include:
- decreased or loss of sense of smell
- blocked or congested nose that does not clear
- pressure or pain behind the nose around the upper teeth
- nosebleeds (particularly if only on one side)
- a lump or sore inside the nose or mouth or on the face.
Other symptoms may include:
- frequent headaches or pain in the sinus areas
- numbness or tingling in the face
- swelling or trouble with the eyes, such as double vision, complete or partial loss of sight, or a bulging or watery eye
- painful or loose teeth (or dentures)
- pain or pressure in the ear
Some people with nasal or paranasal sinus cancers may not experience any symptoms at all. However if you have any of these symptoms for more than a few weeks, talk to your doctor as early as possible. They may be able to help diagnose and treat you.
What are the Tests for Nose Cancer?
It is important that your doctor establishes the diagnosis of Nose Cancer, assesses the size of the cancer and whether it has spread to the lymph nodes in the neck or elsewhere in the body. To answer these questions your doctor will need do the following things:
- talk with you about your medical history. This includes signs you may have noticed, any health conditions, medications that you are taking, and whether you smoke or drink alcohol
- perform a physical examination by feeling and looking inside the nose, face and neck
- order diagnostic tests, which may include scans.
Not everyone will need to have every test for Nose Cancer. Your doctor will recommend tests that are right for you.
Common tests include:
Section title
This involves taking a small piece (sample) from the cancer. A pathologist then looks at the sample under a microscope to check for cancer cells. This is often the only sure way to tell if you have cancer.
Your doctor may recommend an incision biopsy or a needle biopsy.
- Incision biopsy: Your doctor will take a small piece of tissue using a surgical knife. This can be done under topical or general anaesthesia, so that you don’t feel any pain. In both cases, an endoscope and biopsy forcep is used to go through the nose into the nasopharynx. Depending on the size and location of the biopsy, you may need stitches. There may be some bleeding after the biopsy. If you take blood thinners you may need to stop these before the biopsy.
- Needle biopsy (Fine Needle Aspiration or FNA): This is used when there is a lump (enlarged lymph node) in the neck that could have cancer cells in it. During the procedure, your doctor will take some cells from the lump using a needle. Usually this is done with guidance from an ultrasound to make sure the needle is in the right spot. You may feel a bit uncomfortable during the biopsy.
This uses X-rays to take pictures of the inside of the body. If the person has cancer, a CT scan can help your doctor see where it is, measure how big it is and if it has spread into nearby organs or other parts of the body.
MRI (Magnetic Resonance Imaging) Scan
This uses magnetic fields to take pictures of the inside of the body and demonstrates the soft tissues. This helps your doctor see how far a cancer has grown into the tissue around it.
PET (Positron Emission Tomography) Scan
This is a whole body scan that uses a radioactive form of sugar which can show if the nasal or para nasal sinus cancer has spread elsewhere in the body.
Treatment Options for Nose Cancer
Following a diagnosis of Nose Cancer your cancer care team will discuss treatment options including the possibility of participating in a clinical trial that is suitable for you. This is also a good time to consider if you would like a second opinion.
The most suitable treatment for Nose Cancer depends on many things including:
- type of Nasal or Para Nasal Cancer
- size and location of the cancer
- whether the cancer has spread
- personal factors (e.g. age, general health and treatment history)
- types of treatment available (and whether any clinical trials are available)
- your preferences for treatment.
Nose Cancers are generally treated with surgery, radiation therapy, or a combination of both. Radiation therapy may be in combination with chemotherapy (adjuvant concurrent chemoradiation)
Surgery involves taking the cancer out of the nasal cavity and para nasal sinuses and for some people, the lymph glands in the neck. Some people may need extra treatment after surgery to reduce the risk of the cancer coming back.
This can be either radiation therapy alone (adjuvant radiation therapy) or radiation therapy in combination with chemotherapy (this is called adjuvant concurrent chemoradiation).
Surgery for Nose Cancer
There are a number of different operations that can be used to remove Nose Cancer. The operation used will depend on the size, the type nasal cancer and location of the tumour.
How can I prepare for the surgery?
Your doctor will explain details of the surgery, general risks and side effects of surgery. Ask your doctor if you have questions. They may recommend:
- stopping blood thinners (e.g. aspirin) before surgery to reduce the risk of bleeding
- special stockings to reduce the risk of blood clots
- early mobilisation (i.e not staying in bed) to reduce the risk of blood clots and chest infection
- antibiotics to lower the risk of wound infection.
If you smoke, it is important that you consider stopping smoking before starting treatment to help reduce the risk of infection and help you recover after your treatment.
Surgical procedures include:
Download PDF - Endoscopic Sinus Surgery
This is when a telescope and surgical instruments are passed through the nose to get to the nasal cavity, paranasal sinuses, nasopharynx and sometimes into the brain without needing to cut through the skin on the outside.
Download PDF - Craniofacial Resection
This involves removing the cancer using cuts (incisions) via the face and the skull. It is used for cancers that have grown inside, or approach the skull.
Download PDF - Orbital Exenteration
This involves the removal of the eye or eye lid. It is used when the cancer has spread into the eye socket and cannot be treated any other way.
Download PDF - Neck Dissection
Download PDF - Return to Activity Following Neck Dissection
This involves removing lymph nodes from the neck. It is used when the cancer has spread to the lymph nodes in the neck, or there is a risk of microscopic cancer in the lymph glands of the neck.
Reconstructive Surgery (Soft Tissue Free Flap)
Download PDF - Reconstructive Surgery (Soft Tissue Free Flap)
This may be considered if a large area of tissue is removed. Reconstructive surgery may involve taking tissue from another part of the body called a free flap repair. This operation may be carried out by a surgeon who specialises in reconstructive surgery, your head and neck surgeon or another surgeon.
A tracheostomy is used to create an opening in the trachea (windpipe) after major head and neck surgery. A tube is inserted into the opening to help you breathe until normal breathing is possible.
- A gastrostomy tube (called a PEG tube) goes through the skin and the muscles of your abdominal wall into the stomach. Gastrostomy is recommended if feeding is needed for a medium to longer time (months or years).
- A nasogastric tube goes through the nose down into the stomach. Nasogastric feeding is used for short time (days or weeks).
Side Effects of Surgery
Treatment for Nasal and Para Nasal Sinus Cancer may lead to a number of side effects. You may not experience all of the side effects. Speak with your doctor if you have any questions or concerns about treatment side effects.
Radiation Therapy for Nose Cancer
The most common radiation therapy approach for Nose Cancer is called external beam radiation. This type of radiation therapy applies radiation from outside the body.
Radiation therapy can be used in the following ways:
Definitive
This is the main treatment for Nasal and Para Nasal Sinus Cancer. It is used without surgery to cure Nasal and Para Nasal Sinus Cancers.
Definitive radiation therapy can also be given in combination with chemotherapy (called concurrent chemoradiation). The decision to give radiation therapy, alone or in combination with chemotherapy depends on the type of tumour, how big it is and how fit and strong you are. Typically radiation therapy is delivered one each week day (not on weekends) over 7 weeks.
Neo-adjuvant
This is when radiation therapy is given before surgery to help shrink large cancers so they are easier to remove during surgery. Sometimes chemotherapy is added to radiation therapy (chemoradiation) to make it more effective.
Adjuvant
This is when radiation therapy is given after surgery. It is used as an additional treatment to kill cancer cells that may not have been removed during surgery. This typically starts about 4 weeks after surgery to give you time to recover from the surgery. The radiation therapy usually lasts for about 6 weeks. Sometimes chemotherapy is added to the adjuvant radiation therapy (chemoradiation) to make it more effective.
The decision to give radiation therapy, either alone or in combination with chemotherapy, is based on the pathology results after surgery and how fit and strong you are to cope with the treatment. The aim is to lower the risk of the cancer coming back again in the nose, sinuses or neck, however not all patients need this.
Palliative
In cases where a cure is not possible, radiation therapy is used to relieve symptoms of advanced nasal and para nasal sinus cancer. Symptoms that may require palliative radiation therapy include pain, bleeding and pressure symptoms pressing on vital structures (e.g. visual disturbance and headaches).
How do I prepare for Radiation Therapy?
You will meet with many members of the cancer care team, who will help you learn how to look after yourself through radiation therapy, recovery and long term follow-up. They will also talk to you about side effects and how to manage them. It may be helpful to write down questions as they come up, so you can ask anyone in your cancer care team when you see them.
Radiation Therapy Mask-Making and Simulation
- Radiation therapy is a precise treatment. In order to make sure, that the cancer is covered by the treatment, you will need to be very still during the treatment, usually for about five minutes. A radiation therapy mask that is made to fit perfectly to your shape, will be put on you during each treatment to help the machine target where the cancer is.
- You will have a planning CT scan (and sometimes other scans) with the mask on. Your radiation oncologist and radiation therapists will use these scans with all your other clinical information to develop a radiation therapy plan just for you (a personalised plan). Your plan will be checked by the radiation therapy and radiation oncology physics team before it is ready to be used for your treatment. This whole process can take approximately 2-3 weeks.
Teeth and Mouth Care
You might need to have some of your teeth taken out, this will depend on the area being treated and the dose of radiation therapy. It is important to take out any broken or infected teeth before radiation therapy. Taking out unhealthy teeth after radiation therapy can cause problems with the jaw bone. Further information about removing teeth and what to expect before and after the operation is available here.
Diet and Nutrition
Your cancer and its treatment can make it hard to eat and drink. Your doctor will recommend you see a dietitian to maximise your nutrition during treatment as well as while you are recovering. Sometime feeding tubes may be recommended depending on the area being treated and the dose of radiation therapy.
There are two common types of feeding tubes:
- Gastrostomy tube (sometimes called a PEG tube): this type of tube is inserted through your abdominal wall into your stomach, with part of the tube staying outside the stomach. A syringe can be attached to the tube to give you food this way if needed. The tube is inserted using a camera through the mouth into the stomach (gastroscopy) or using a CT scanner to guide insertion directly through the skin. If a PEG tube is needed, your doctor will organise this before starting your radiation therapy
- Nasogastric tube: this type of tube goes through the nose down into the stomach and is usually used for short periods (days or weeks). A nasogastric tube can be inserted at any time (before, during or after treatment).
Speech, Voice, Swallowing
Your cancer and its treatment can make swallowing and speech difficult. Your doctor will recommend you see a speech pathologist, who can help you with ways to manage swallowing and communication difficulties, during and after treatment.
There are many other aspects of supportive care that are available, ask your doctor if you have any specific needs.
Side EffectsThe side-effects of radiation therapy start around two weeks into treatment and progress through treatment to peak in the last week or just after treatment ends. The side effects start to improve 2-3 weeks after the end of treatment.
Side effects associated with radiation therapy depend on:
- the dose of radiation therapy
- the area being treated
- whether or not chemotherapy is added to the radiation.
Each person responds to radiation therapy differently. Some people may experience a few side effects while others may not experience any at all. The following are some common side effects of radiation therapy.
Common side effects of radiation therapy include:
- tiredness
- skin irritation in the treated area e.g. redness, dryness and itching, weeping skin, scaling or sometimes skin breakdown (sores)
- nasal irritation, blockage and crusting
- dry mouth and throat due to lack of saliva (called xerostomia)
- altered taste, which is usually a loss of taste or sometimes an unpleasant taste in the mouth
- pain on swallowing or difficulty with swallowing.
Most side effects are short lived and may go away within 4–6 weeks of finishing radiation therapy. Some side effects may last for months after you finish radiation therapy and some may be permanent.
Rare side effects from nerve damage (called cranial neuropathy) may occur following treatment of very advanced cancers. These include difficulty speaking, swallowing, impaired and double vision. The nasal and paranasal cavity is very close to a number of important structures such as the spinal cord, brain and nerves involved with vision, hearing and balance. Your radiation oncologist will be very careful to avoid these structures by using very precise radiation therapy techniques but sometimes rare side effects may occur from the radiation therapy. You can talk to your radiation oncologist to find out if these concerns apply to your situation and to find out more about these rare side effects.
Once your radiation therapy ends, you may continue to have follow-up appointments so that your doctor can check your recovery and monitor any side effects that you may have. Sometimes your doctor may arrange for a PET scan about 12 weeks after finishing radiation therapy to make sure the cancer has completely gone.
Your doctor may recommend that you receive specific supportive care to help during your treatment and recovery.
Chemotherapy for Nose Cancer
Chemotherapy works by destroying or damaging cancer cells. For Nasal and Para Nasal Sinus Cancers, it is usually given into a vein through a needle with a cannula (tube) attached.
There are a number of ways that chemotherapy may be used to treat Nose Cancer including:
Definitive
Sometimes chemotherapy is added to definitive radiation therapy (chemoradiation). This may be given once every 3 weeks or once a week throughout the duration of radiation therapy. This makes the radiation more effective at killing cancer cells but also leads to more side effects in most people.
Adjuvant
This is when chemotherapy is given after surgery and is usually combined with radiation therapy (called concurrent chemoradiation). This may be given once every 3 weeks or once a week throughout the duration of radiation therapy. This makes the radiation more effective at killing cancer cells but also leads to more side effects in most people. Unlike chemotherapy for many other cancers, most people do not lose their hair or have severe nausea and vomiting.
Neo-adjuvant
This is when chemotherapy is given before surgery or radiation therapy. It works to shrink large cancers so they are easier to remove during surgery or target with radiation therapy
Palliative
This is used when the cancer is incurable. The cancer may be too large or has spread too much to be removed by surgery. Palliative chemotherapy helps to slow the growth of cancer and reduce symptoms. It is important to remember that palliative chemotherapy is not as intense as other types and is much less likely to have significant side effects.
Before you start treatment, your medical oncologist will choose one or more chemotherapy medications that will be best to treat the type of cancer you have.
The chemotherapy medications your doctor chooses may depend on:
- whether the treatment is curative or palliative
- when it is used
- your medical history.
Side Effects
The side effects of chemotherapy depend on the medication used and and how much you are given by your doctor (the dose). The most common medications used are called cisplatin, carboplatin and cetuximab.
Each person responds to chemotherapy differently. Some people may experience a few side effects while others may not experience any at all.
The following are common side effects of chemotherapy:
- nausea and vomiting
- more side effects of radiation, if you have chemotherapy at the same time as radiation
- loss of feeling in the fingers and toes
- some medications may cause kidney damage
- hearing loss/thinning
- ringing in the ears
- rash
- higher risk of infection (if the chemotherapy reduces the number of white cells in the blood).
Most of these side effects are short lived and may go away once you finish chemotherapy. . Some side effects can take months or years to improve or may be permanent
Once your treatments end, you will have regular follow-up appointments so that your doctor can check your recovery, make sure the cancer has not returned and monitor and treat any side effects that you may have.
Your doctor may recommend that you receive some specific supportive care to help during your recovery.
Questions to ask
- Exactly what type of Nose Cancer do I have? Where is it located?
- Why did I get this cancer? Is it related to smoking or alcohol?
- Why did I get this cancer? Is it related to the HPV virus?
- What stage is the cancer?
- What are my treatment options? Which treatment do you recommend for me and why?
- Have you discussed my case at a Multidisciplinary Team meeting and what were the recommendations?
- Who will be part of the cancer care team, and what does each person do? Should I see another specialist before treatment, such as a radiation oncologist, medical oncologist, plastic surgeon, dentist, dietitian or speech pathologist?
- What are the possible side effects of treatment in the short- and long-term? How can they be prevented or managed?
- Will the treatment affect my ability to eat, swallow, or speak? Will I need a feeding tube?
- What will happen if I don't have any treatment?
- How much will the treatment and/or operation cost? Will Medicare or my health insurance cover it?
- What follow-up tests will I need? How often will they be?
- Am I suitable for any clinical trials?
- What lifestyle changes (diet, exercise) do you recommend I make?
- Who can I call if I have any problems or questions?
- Where can I find emotional support for me and my family? Is there a support group or psychologist you can recommend?
- If I wanted to get a second opinion, can you provide all my medical details? Do you mind if I get a second opinion?
Follow-Up Care
You will need regular check-up of your face, mouth, throat and neck after treatment for Nasal and Para Nasal Sinus Cancer. This may include endoscopic examinations and imaging such as CT, MRI and PET scans, during follow-up. It is important to keep up with follow-up appointments to make sure that if the cancer comes back it is caught early and can be treated. If you have any concerns between appointments you should contact your doctor.
People who smoke and/or drink alcohol can reduce the risk of their cancer coming back or getting a new cancer if they quit smoking and reduce the amount of alcohol they drink. Ask your cancer care team for advice if this applies to you.
Mental health for people with Cancer
Sometimes this is referred to as psychosocial aspects or survivorship.
Being diagnosed with cancer and having treatment can lead to extra worries or concerns for you and the people caring for you. Depending on the treatment, you may experience any of the following:
- low mood or depression
- anxiety
- disfigurement
- difficulties with eating
- difficulties with speaking
- changes in sexual activity
You may have got through the diagnosis and treatment for mouth cancer, but you may be finding it difficult to deal with some of the side effects of treatment. Speak with you doctor about any difficulties you may be experiencing. Your doctor may give you a referral to a psychologist or another healthcare professional who can help you.
For more information about coping with cancer visit Cancer Council Australia.








On this page
